
What Is an AED? (Automated External Defibrillator Guide)
Defibrillators look nothing like what television suggests. The image that stuck from decades of medical dramas features metal paddles, someone shouting “Clear!”, a patient jolted off a table. That image is at least thirty years out of date. The machine that replaced those paddles is lighter than a laptop, speaks out loud, and was designed from the ground up so that the person holding it does not need a medical degree to use it correctly.
That machine is the AED, short for automated external defibrillator. You have probably passed one in a hallway at AdventHealth or a corridor at Orlando International Airport without giving it a second look. The gap between knowing the box exists and knowing what to do when it comes off the wall is wider than it needs to be. That gap can close quickly with a basic understanding of what the device does.
An AED does not replace CPR, and it does not require a doctor standing beside it. It is built to guide the person already there through one of the most critical parts of the cardiac-arrest response.
Educational note: use this information for general awareness only. It is not a substitute for calling 911, hands-on training, or professional medical judgment during an emergency.
Upcoming CPR Class Dates and Times
What Does AED Stand For?
AED stands for automated external defibrillator. The name sounds technical, but each word describes exactly what the device does.
Automated means the machine analyzes the rhythm on its own. External means the pads go on the outside of the chest, not inside the body. Defibrillator means it can deliver a shock when the heart rhythm is one that may respond to defibrillation.
The name “defibrillator” covers only part of what these devices do. A public AED is a guided response tool. Once the pads are attached, it reads the heart rhythm on its own, tells you clearly whether a shock is warranted, and keeps directing the response regardless of what it finds. No clinical judgment is required from the person holding it. The machine handles that part.
What Is an AED and How Does It Work?
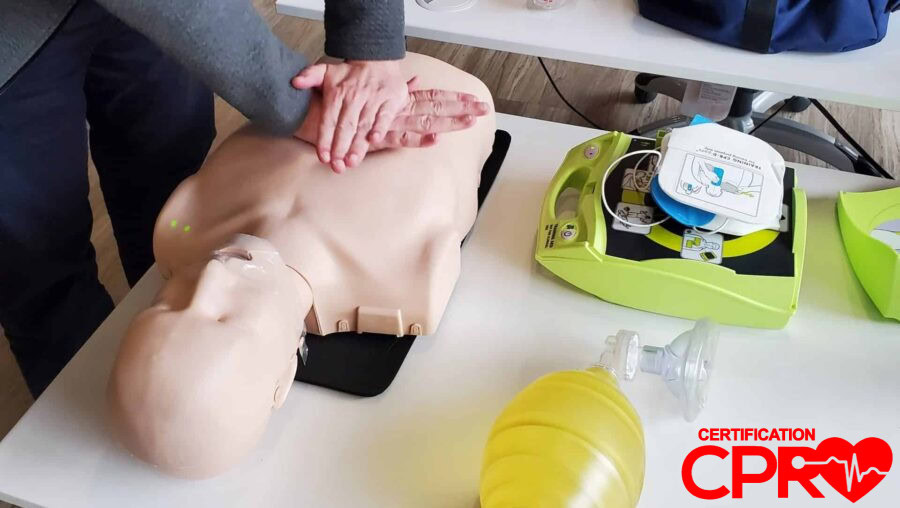
An AED is a portable device used during sudden cardiac arrest: when a person collapses, becomes unresponsive, and stops breathing normally or is only gasping. Once you turn it on, it walks you through the response out loud.
You attach the pads to the bare chest, step back, and let the machine analyze the rhythm. Depending on what it finds, it either prompts you to deliver a shock or directs you back to CPR. Either way, the device keeps you moving at exactly the moment most bystanders would otherwise freeze.
CPR and the AED work together rather than as alternatives. CPR keeps blood moving to the brain and vital organs while the AED assesses whether the heart is in a rhythm that may respond to a shock. The rescuer does not have to make that clinical judgment. The device makes it.
An AED also does not shock every unresponsive person. It only advises a shock when the rhythm matches the specific patterns it is designed to recognize. That built-in intelligence is exactly what makes the device appropriate for public use.
If you want the full CPR-AED sequence to feel less abstract, the hands-on AHA BLS class is the better next step. Reading clarifies the concept; practice makes the response feel natural under pressure.
What Does an AED Look Like?
Most public AEDs are housed in bright red, orange, or yellow wall cabinets, usually labeled with the international AED sign, a green symbol with a heart and a lightning bolt. When you open the cabinet, the device itself is small and rectangular, roughly the size of a thick hardcover book. The pads are stored with it, and most units begin speaking as soon as the lid is opened or the power button is pressed.
In Orlando, AEDs are required by Florida law in health clubs and fitness centers. You will also find them at Orlando International Airport, Disney parks, AdventHealth and Orlando Health facilities, and most large hotels along International Drive and in the convention center area. The best time to notice where the nearest one is mounted is before anybody needs it.
Who Can Use an AED?
Public AEDs are specifically designed for non-medical responders. Cardiac arrest does not schedule itself around who happens to be nearby. The first person at the scene is whoever was already in the room: the person at the front desk, the coworker two cubicles over, a parent in the school pickup line. The AED is on the wall because the response has to begin before EMS can physically get there.
Training still matters. Someone who has practiced the CPR-AED sequence in a hands-on class typically recognizes the emergency faster, moves through the steps with less hesitation, and wastes less time on doubt. But the entire design of a public AED assumes the user may not be a clinician. It is built to coach, not to intimidate.
For workplaces and groups that want their team to know not just where the AED is but how to use it as part of one coordinated response, onsite CPR training is usually the most practical path.
When to Use an AED
You use an AED when a person may be in sudden cardiac arrest: collapsed, unresponsive, and not breathing normally or only gasping. When you see that combination, the decision is already made. Call 911, start CPR, and send someone for the AED at the same time. Once the device arrives, turn it on and follow the prompts.
Upcoming CPR Class Dates and Times
It also helps to know when the AED does not belong in the response. Chest pain alone, dizziness, or someone who is awake and breathing normally calls for a different kind of help. The AED enters the scene when the person has gone down and normal breathing is absent or clearly abnormal.
Every minute of cardiac arrest without CPR and defibrillation narrows the window for a good outcome. The response that works best is also the clearest: recognize the emergency, call 911, start CPR, get the device, and keep following the machine until EMS takes over.